Regarding Coronary Microvascular Dysfunction
Professor Shimokawa, the representative of this research group, has reported on the molecular mechanisms of coronary microcirculatory regulation through his research at Kyushu University and Tohoku University. In this section, we will explain the endothelial function regulatory factors and vascular smooth muscle regulatory factors that have been elucidated by Professor Shimokawa and colleagues to date.
Endothelial cells produce and release vasodilatory factors collectively termed endothelium-derived relaxing factors (EDRF) to maintain vascular homeostasis. EDRF comprises three types of factors: vasodilatory prostaglandins represented by prostacyclin (PGI2), nitric oxide (NO), and endothelium-derived hyperpolarizing factor (EDHF), which were discovered and identified in that order. Professor Shimokawa's research revealed that the contribution of these EDRFs to the vasodilatory response varies significantly depending on vessel diameter, a universal phenomenon independent of animal species or organ. While prostaglandins exert a consistent effect on the vasodilatory response regardless of vessel diameter, NO contributes significantly to the vasodilatory response in relatively large vessels. As vessel diameter decreases, the contribution of EDHF to vasodilation increases. In small arteries (resistance vessels such as coronary microvessels), EDHF becomes the primary mechanism, maintaining physiological balance (Figure 2; Reference 5). Therefore, when considering endothelial dysfunction in coronary microcirculatory disorders, it is essential to consider not only NO but also EDHF. EDHF varies depending on the animal species and vascular bed. However, Professor Shimokawa and colleagues were the first in the world to identify that one of the core components of human EDHF is hydrogen peroxide (H₂O₂), produced at physiological concentrations by the vascular endothelium (Figure 3; Reference 5). To date, it has been established that in coronary microcirculation, H₂O₂ primarily functions as a vasodilator, playing crucial roles in coronary autoregulation, protection against ischemia-reperfusion injury, and tachycardia-induced metabolic vasodilation. Furthermore, it has been demonstrated that in peripheral vessels (digital arterioles) of patients with microvascular angina, vasodilation mediated by NO and EDHF is markedly impaired. This suggests that patients with coronary microcirculatory dysfunction may have systemic microcirculatory impairment, not limited solely to coronary artery disease.
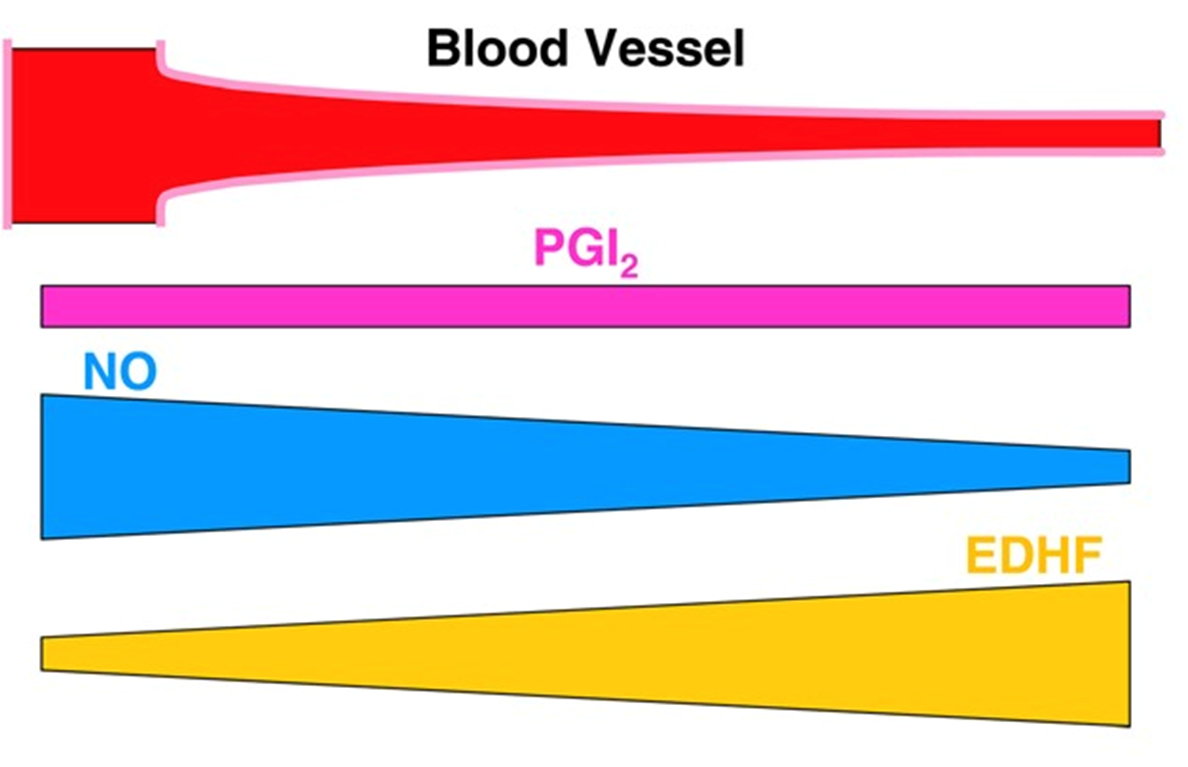
Figure 2: Degree of involvement of three types of endothelium-derived relaxing factors (EDRF) in endothelial function (quoted from Reference 5): Prostacyclin (PGI₂) is mildly involved regardless of vessel diameter, whereas nitric oxide (NO) plays a crucial role mainly in larger vessels. The role of endothelium-derived hyperpolarizing factor (EDHF) increases as the vessel diameter decreases.
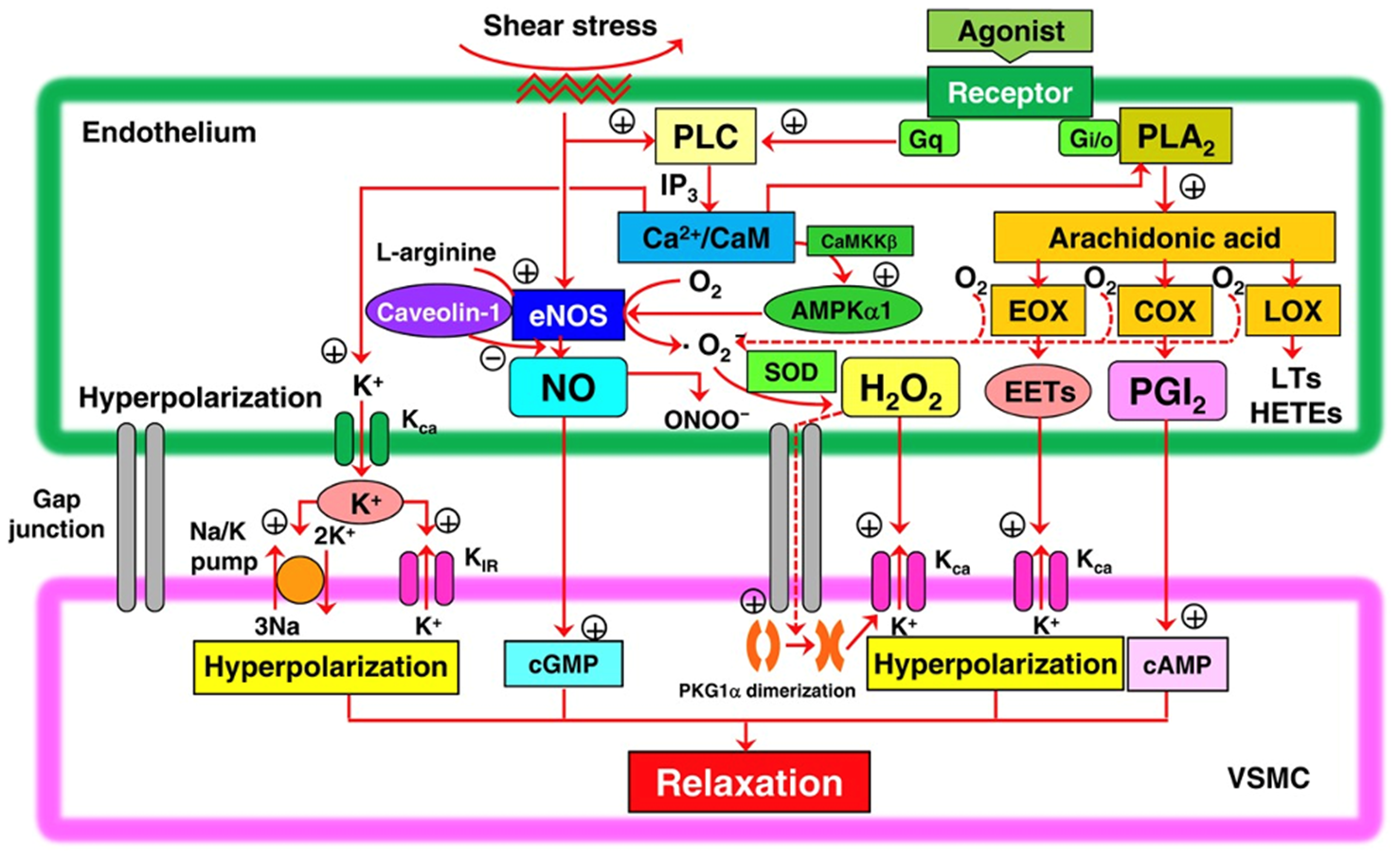
"One of the main components of EDRF is hydrogen peroxide (H₂O₂) (quoted from Reference 5): Endothelial nitric oxide synthase (eNOS) in vascular endothelial cells produces nitric oxide (NO) and superoxide anion (O₂⁻) under physiological oxygen tension conditions. The superoxide anion (O₂⁻) is converted into hydrogen peroxide (H₂O₂) by Cu,Zn-superoxide dismutase (SOD), which functions as a relaxing factor known as endothelium-derived hyperpolarizing factor (EDHF)."
Coronary spasm angina, represented by resting angina, primarily occurs due to transient hypercontraction of vascular smooth muscle in the large coronary arteries of the heart. Through basic and clinical research, Professor Shimokawa, the representative of this research group, and colleagues have revealed that the low-molecular-weight GTP-binding protein Rho and its effector molecule Rho-kinase play a crucial role as switches promoting vascular smooth muscle contraction in the pathogenesis of coronary vasospasm (Figure 4; Reference 5). The contraction and relaxation of vascular smooth muscle are determined by the balance between myosin light chain kinase (MLCK) activity and myosin light chain phosphatase (MLCPh) activity, with the phosphorylation of myosin light chain (MLC) playing a central role. While it has long been known that these processes are regulated by intracellular Ca²⁺ concentration, it has been discovered that Rho-kinase, as mentioned above, controls the contraction and relaxation of vascular smooth muscle independently of intracellular Ca²⁺ concentration. Rho-kinase inhibits the activity of the myosin-binding subunit of MLCPh by phosphorylating it. This disrupts the balance between MLCK and MLCPh activity, leading to increased phosphorylation of MLC and consequently causing vascular smooth muscle contraction. Coronary vascular resistance contributed by the large coronary arteries on the heart surface is said to account for only about 5% of total coronary vascular resistance. Vascular resistance generated by the coronary microcirculation plays a central role in regulating myocardial blood flow. This implies that myocardial ischemia can be induced by impaired regulation of the coronary microcirculation, regardless of the presence or absence of stenosis in the large coronary arteries or coronary vasospasm.
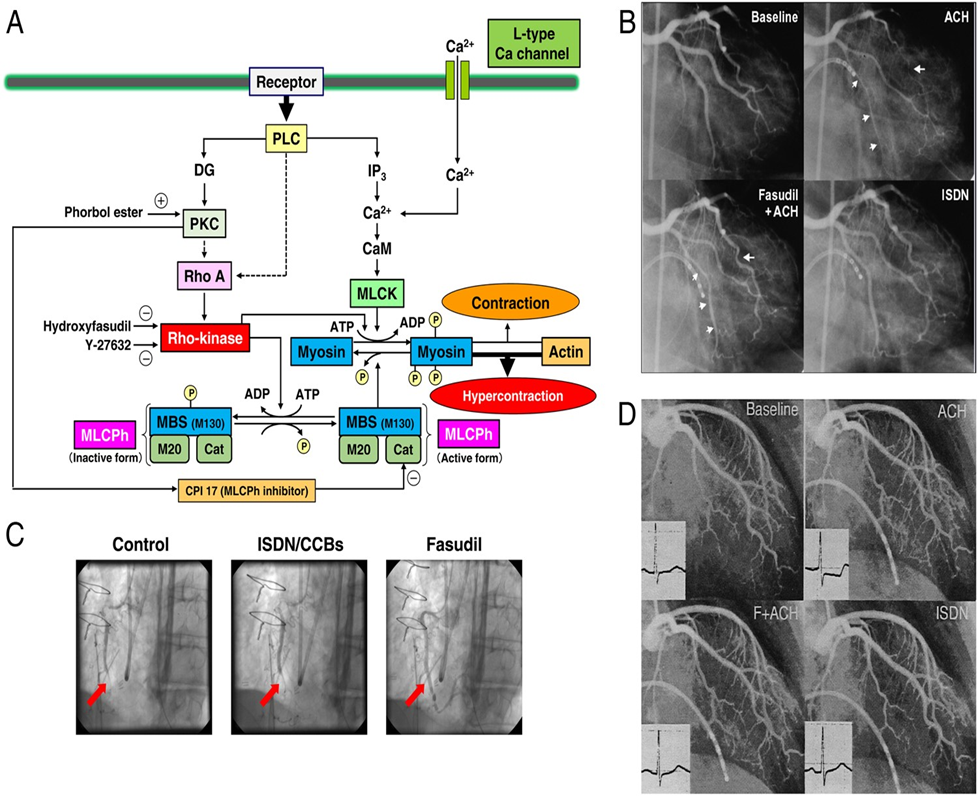
Figure 4. Molecular mechanisms of coronary spasm-induced vascular smooth muscle hypercontraction (quoted from Reference 5):
(A) The central role in the molecular mechanism of vascular smooth muscle hypercontraction is played by the enhancement of myosin light chain phosphorylation, mediated through inhibition of myosin light chain phosphatase (MLCP) by Rho kinase.
(B) In patients with vasospastic angina, multibranch coronary spasm induced by acetylcholine (ACH) was suppressed by pre-administration of the Rho kinase inhibitor fasudil.
(C) Coronary spasm refractory to both calcium channel blockers (CCBs) and nitrates (isosorbide dinitrate, ISDN) after coronary artery bypass surgery was suppressed by intracoronary injection of fasudil.
(D) In patients with microvascular angina, ischemic electrocardiographic changes induced by acetylcholine (ACH) were suppressed by pre-administration of the Rho kinase inhibitor fasudil (F + ACH).
In addition to the vascular endothelial dysfunction described in section 4-1) above, another major factor contributing to coronary microcirculatory abnormalities is considered to be vascular smooth muscle dysfunction, as discussed in this section. Recently, Professor Shimokawa and colleagues from Tohoku University, representing our society, reported that the coexistence of coronary vasospastic angina and elevated microvascular resistance index, indicative of microvascular dilation dysfunction, is associated with worsened cardiac prognosis (Figure 5; Reference 6). A common underlying mechanism is thought to involve dysfunction of Rho kinase. One of the goals of this research group is to disseminate evidence supporting this hypothesis.
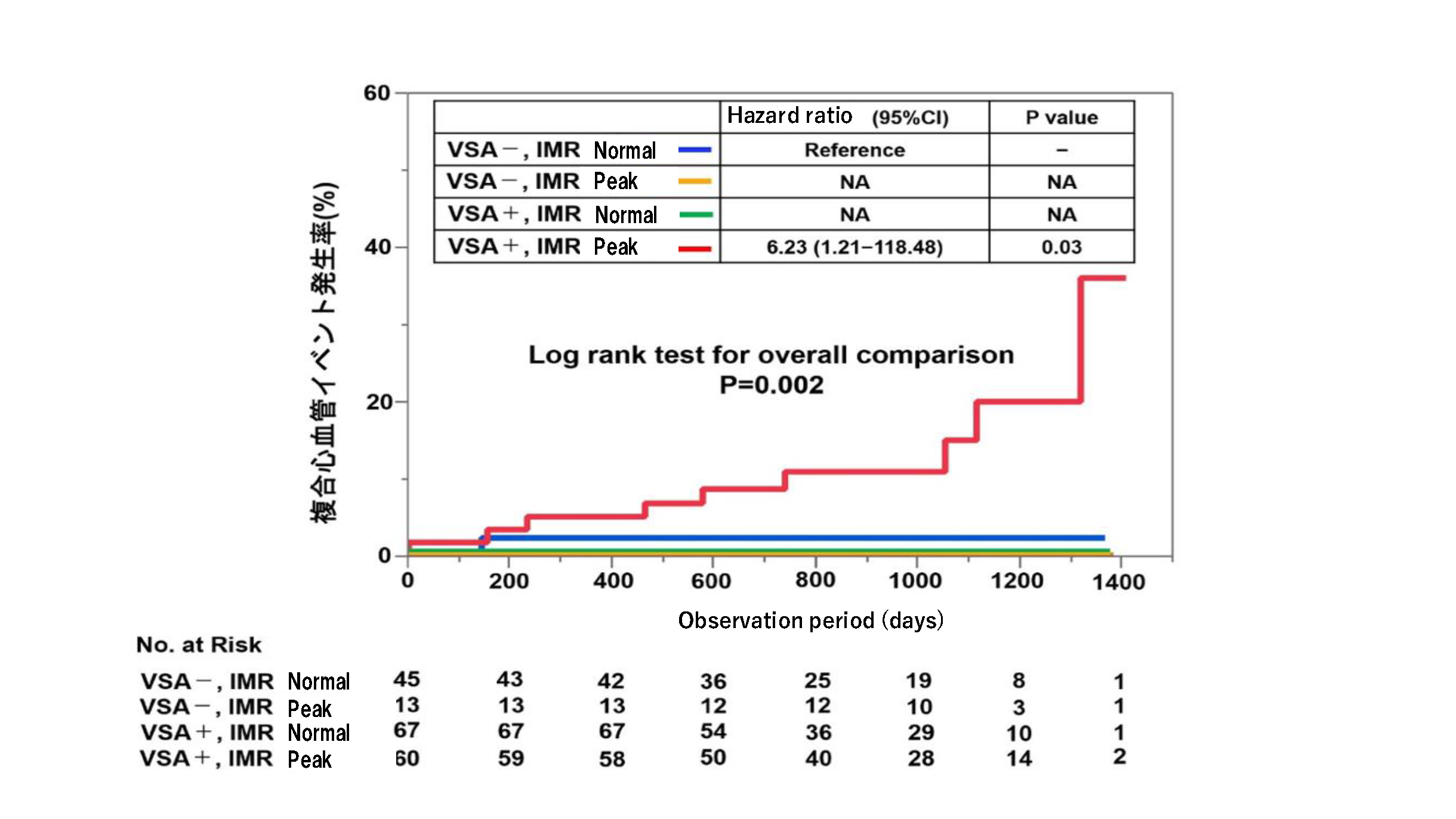
Figure 5. Examination of long-term treatment outcomes based on the presence or absence of coronary spasm on the heart surface and the high or low microvascular resistance index (IMR) (modified and cited from reference 6): Patients were classified into four groups based on the presence or absence of coronary spasm on the heart surface (VSA) and the high or low IMR (cutoff value = 18). The incidence of composite cardiovascular events (including hospitalization due to unstable angina or myocardial infarction, and cardiac death) was then examined. The group with both coronary spasm on the heart surface and high IMR (VSA+; high IMR: red line) showed a significantly higher incidence of composite cardiovascular events compared to the other groups.
References
5) Eur Heart J 2014;35:3180-93
6) J Am Coll Cardiol 2019;74(19):2350-60

© 2022 日本冠微小循環障害研究会