Examination methods and treatments
The etiology of coronary microvascular dysfunction involves both an exaggerated vasoconstrictive response and a diminished vasodilatory response of the coronary microvasculature, as well as the involvement of both factors (Reference 1 see Figure 6). It is necessary to examine these two aspects in detail during cardiac catheterization. The exaggerated vasoconstrictive response can be evaluated using a coronary spasm provocation test (acetylcholine loading test), while the reduced vasodilatory response is assessed through coronary flow reserve.
Acetylcholine is gradually injected into the coronary arteries to induce coronary spasm. The spasm of the large coronary arteries on the heart surface is evaluated via coronary angiography. Simultaneously, a catheter is inserted into the coronary sinus, which is the outflow tract of the coronary circulation, and blood samples are taken from two sites: the entrance of the coronary circulation at the ascending aorta. This allows for the assessment of coronary microvascular spasm (see Figure 8).
In the absence of myocardial ischemia, the myocardium consumes lactate from the blood, resulting in lower lactate levels in the coronary sinus compared to the entry point. However, when myocardial ischemia occurs, the myocardium produces lactate, causing the lactate level in the coronary sinus to become higher than at the entry. The reversal of lactate levels is considered the most sensitive indicator of myocardial ischemia.
If lactate reversal (indicating myocardial ischemia) occurs without spasm in the large coronary arteries, it is evaluated as the induction of coronary microvascular spasm.
To assess the vasodilatory capacity of the coronary microvasculature, a specialized wire is directly inserted into the coronary artery. Evaluation is performed using a heat dilution method with a pressure sensor combined with a temperature sensor.
In order to determine coronary microcirculatory indices, it is necessary to obtain information on intracoronary pressure and coronary blood flow both at rest and in a state where coronary microcirculation is maximally dilated (maximal hyperemia). By combining these data, coronary microcirculatory indices can be calculated. The main indices include:
① Coronary Flow Reserve (CFR)
② Index of Microvascular Resistance (IMR)
(Refer to Figure 9).
It is primarily determined by using pharmacological agents such as adenosine to induce maximal hyperemia, and calculating the ratio of the maximum coronary blood flow during this state to the resting coronary blood flow. In other words, it is an indicator that reflects the heart's ability to increase coronary blood flow in response to increased myocardial oxygen demand.
While FFR (Fractional Flow Reserve) and Resting Index are used to assess whether significant stenosis (which could cause ischemia) exists in the epicardial coronary arteries, CFR represents a measure of the entire coronary circulation, including both the epicardial coronary arteries and the coronary microcirculation. Therefore, to evaluate only the coronary microcirculation using CFR, it is necessary that there are no significant stenoses in the epicardial coronary arteries.
A normal CFR value is considered to be 2.0 or higher. Conditions that can lead to a decreased CFR include the presence of significant stenosis that restricts blood flow in the epicardial arteries, increased resting blood flow, and suppressed increase in coronary blood flow during maximal hyperemia. Since CFR is calculated as the ratio of coronary blood flow during maximal hyperemia to that at rest, it can sometimes be difficult to determine whether the abnormality is due to issues at rest or during hyperemia. In such cases, the Index of Microcirculatory Resistance (IMR) can be a useful additional measure.
R is an indicator that reflects the maximum coronary microvascular resistance during hyperemia, calculated by dividing the coronary pressure by the coronary blood flow in the state of maximal hyperemia. IMR represents the pressure involved in the coronary microcirculation, indicating how much blood flow passes when this pressure is applied. An IMR value of 25 or below is considered normal.
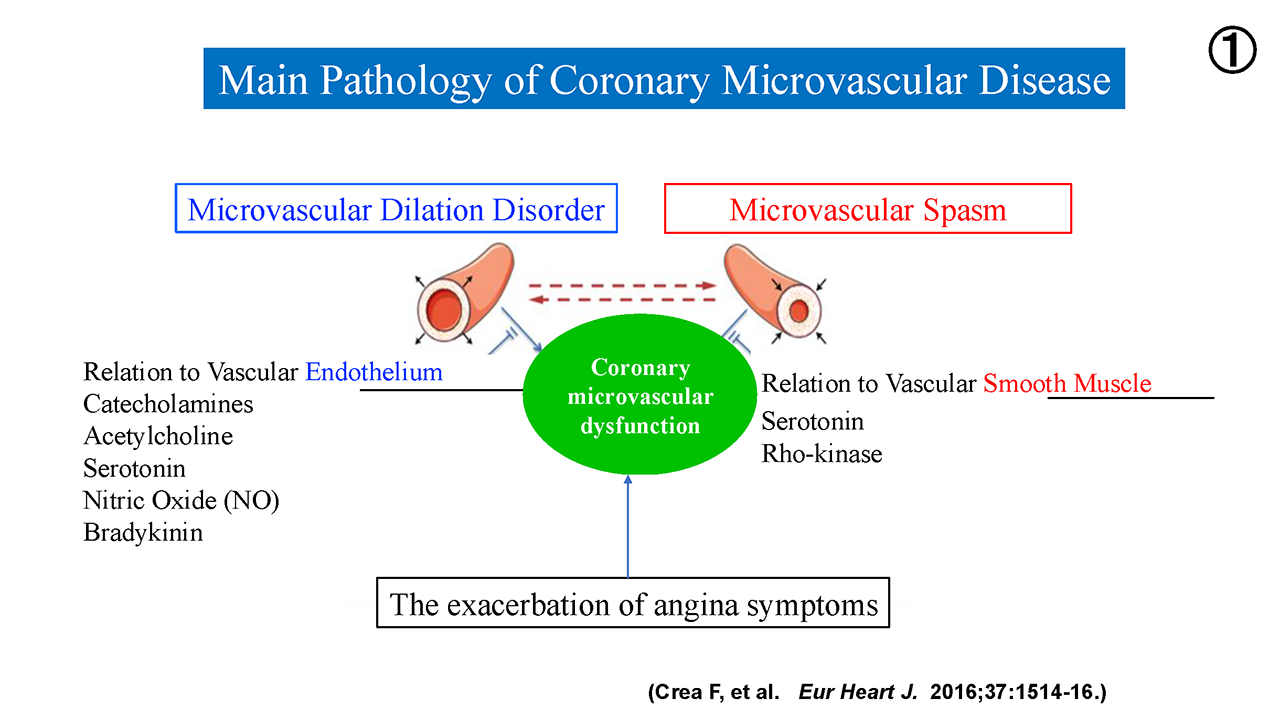
Figure 6:Main Pathology of Coronary Microvascular Disease
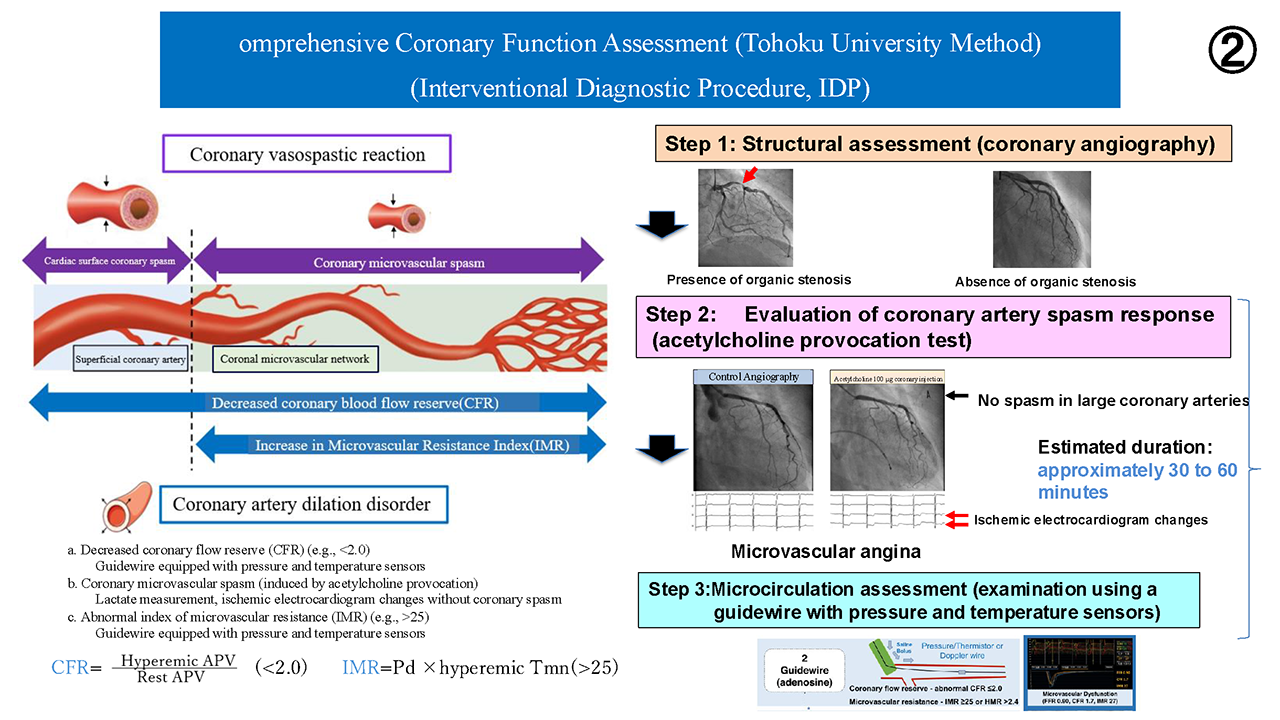
Figure 7:omprehensive Coronary Function Assessment (Tohoku University Method)
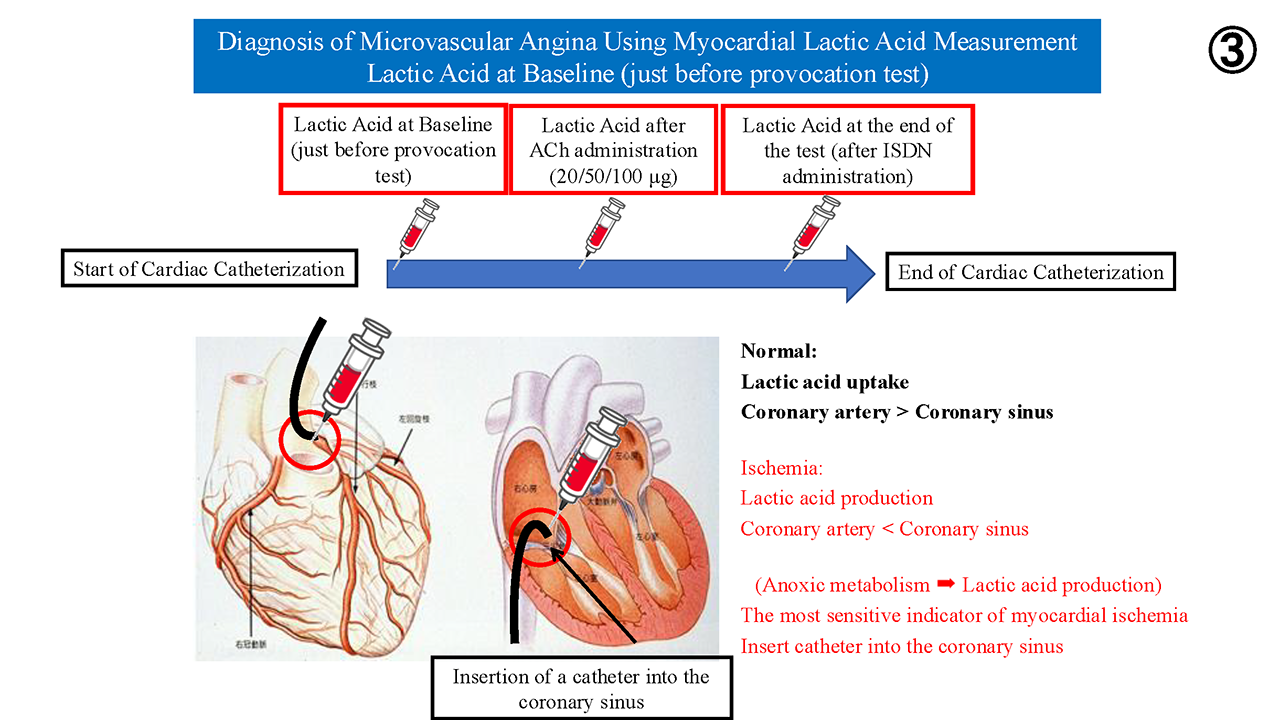
Figure 8:Diagnosis of Microvascular Angina Using Myocardial Lactic Acid Measurement
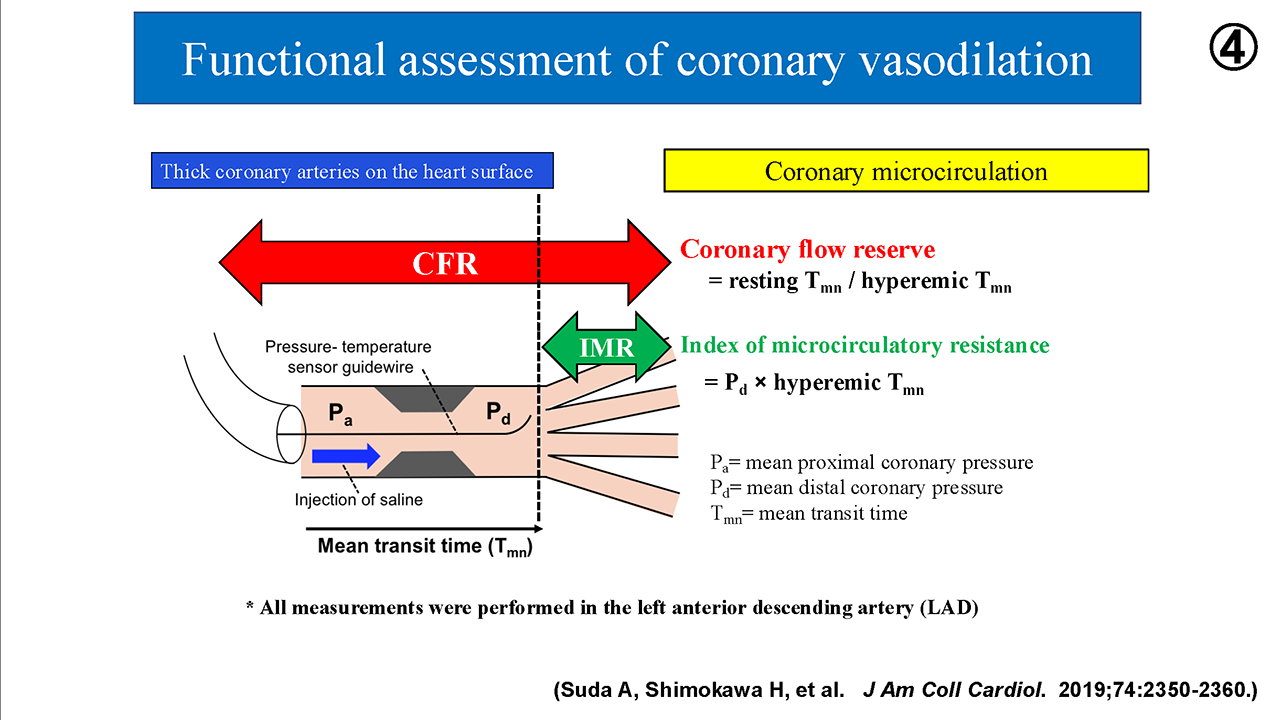
Figure 9:Functional assessment of coronary vasodilation

© 2022 日本冠微小循環障害研究会